

Introduction:
Cardiac lymphomas are very rare with diffuse large B-cell lymphoma (DLBCL) considered to be the most common histology. These lymphomas can be either local "primary cardiac" disease, or part of dissemination by systemic lymphoma. There is limited data regarding outcomes of patients with this disease. We sought to evaluate the outcomes of cardiac DLBCL in both pre- and rituximab eras using a large retrospective database.
Methods:
The public Surveillance, Epidemiology and End Results (SEER) database was used to identify all patients diagnosed with DLBCL and heart as the primary disease site. Data cutoff in the database was in 2016. Patients with missing date of diagnosis or survival data were excluded. Patients were divided into two groups based on diagnosis year, with rituximab cohort included all DLBCLs diagnosed in 2006 and later (2006 was FDA approval year of rituximab in untreated DLBCL). Treatment effect (surgery, radiation, chemotherapy) was analyzed when available. survival was estimated using the Kaplan-Meier method, and compared using Log-Rank test. Cox proportional hazards models were used for adjusted survival analyses.
Results:
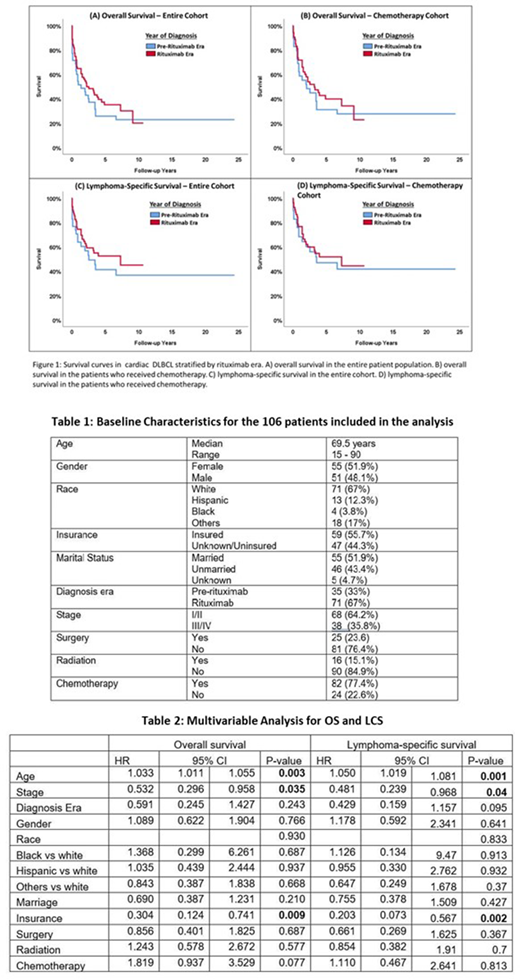
Total of 106 patients were included in the final analysis, baseline characteristics are summarized in table 1. Median age at diagnosis was 69.5 years with only about 10% of patients being 50 years or younger. Most patients were white 71 (67%), had local stage I/II disease 68 (64.2%), and belonged to the rituximab era group 71 (67%). Most patients had chemotherapy 82 (77.4%), while only 25 (23.6%) had surgery, and 16 (15.1%) had radiotherapy. Median overall survival (OS) for the entire cohort was 22 months (0-292). Median OS was 16 months (95% CI, 0.55 -31) for the pre-rituximab group, and was 26 months (95% CI, 7.5 - 45) for the rituximab group which were not statistically different (p-value =0.340). Median lymphoma-specific survival (LCS) was 30 months (95% CI, 8.0 -52) for the pre-rituximab group, and was 36 months (95% CI, 16 - 158) for the rituximab group which were not statistically different (p-value =0.295). OS and LCS were also not different between the two era groups when stratified by chemotherapy (figure 1). On univariate analysis, Chemotherapy was associated with better OS [HR = 0.472, 95% CI (0.277-0.806); p-value = 0.006] but not LCS [HR = 0.690, 95% CI (0.341-1.396); p-value = 0.302]. Using a multivariate analysis model, both OS and LCS were associated with lymphoma stage, insurance status and age but not with diagnosis era or chemotherapy (table 2).
Conclusion:
Cardiac DLBCLs are rare and affecting mostly the elderly. No significant improvement in outcomes were noted in the current rituximab era. Age, disease stage, and having health insurance were associated with better outcomes. The role of chemotherapy needs further evaluation in larger studies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal